Editor’s note: This text-based course is a transcript of the webinar, Power Wheelchairs, presented by Michelle Lange, OTR, ABDA, ATP/SMS.
Learning Outcomes
- After this course, participants will be able to:
- identify clinical indicators for scooters and power wheelchairs.
- list 3 types of power seating.
- identify 2 categories of power wheelchair alternative driving methods.
Introduction
Welcome, everyone. I hope this course is helpful to you and especially to the clients with which you work. Today, we will discuss power wheelchairs. As we go through this information, you will see that this is an overview of this topic. If you want to dive down even deeper, we have many other related power mobility topics available through OccupationalTherapy.com.
What We Are Covering
- Mobility Series
- Augmented Mobility
- Dependent Mobility
- Manual Mobility
- Power Mobility
This is part of a series reviewing mobility categories including Augmented Mobility, Dependent Mobility, Manual Mobility, and today Power Mobility. I would encourage you to check out these other offerings.
Power Mobility Devices
- Power Operated Vehicles (POVs)/Scooters
- Power Wheelchairs
- Provide independent mobility using a motorized mobility base
Power mobility devices include power operated vehicles (POVs) or scooters and power wheelchairs. Each of these provides independent mobility for the driver using a motorized mobility base.
- Goals of use include:
- Providing independent mobility to a client who:
- Is unable to self-propel any manual wheelchair
- Is unable to self-propel any manual wheelchair efficiently
- Safely
- Timely
- Without undue fatigue and/or effort
- Without undue cardiopulmonary effort
- Providing independent mobility to a client who:
Power mobility devices provide independent mobility to a client who is unable to self-propel any type of manual chair. It is important to emphasize "any type" of a manual wheelchair because there are a variety of options covered in the aforementioned prior course. It might be that a client could be successful with a manual wheelchair if they had the appropriate category. The client may be able to self-propel a manual chair but not efficiently. How long does it take a person to get from point A to point B? We also need to consider if the client can propel safely and without undue fatigue and cardiopulmonary effort. Some clients are capable of propelling a manual chair, but it is at a great metabolic cost to their bodies. We need to be aware of that as well.
- Who uses this technology?
- Clients with the diagnosis of:
- High-level spinal cord injuries
- TBI
- CP
- Muscle diseases
- DMD
- SMA
- Neuromuscular diseases
- ALS
- MS
- Clients with the diagnosis of:
Who utilizes this technology? Clients with the following diagnoses typically use power mobility such as high-level spinal cord injuries, traumatic brain injuries, cerebral palsy, and muscular diseases, such as Duchenne muscular dystrophy, spinal muscular atrophy, ALS, and MS. Not every person with these diagnoses requires a power wheelchair, but often these are diagnoses where we are going to consider power mobility.
Assessment
- Assessment is typically done with a wheelchair supplier
- Many Power Wheelchairs are considered Complex Rehab equipment
- Complex Rehab is typically recommended by a professional who is certified:
- ATP: Assistive Technology Professional
- SMS: Seating and Mobility Specialist
- These are obtained through RESNA
- Rehab Engineering and Assistive Technology Society of North America
The assessment determines if someone is an appropriate candidate for a power wheelchair and what specifically is required for that individual. The assessment is done between the clinician and a wheelchair supplier.
Many power wheelchairs are complex rehab equipment and require a very experienced team to make these recommendations. Sometimes the funding source will require certain credentials before allowing someone to participate in these evaluations, particularly the supplier. Complex rehab equipment is typically recommended by someone who is a certified Assistive Technology Professional or ATP. This certification is through an organization called RESNA, the Rehab Engineering and Assistive Technology Society of North America. There is also a secondary certification called the SMS or Seating and Mobility Specialist. The SMS certification is not typically required for funding but does demonstrate that the individual has achieved a certain amount of experience, more advanced skills, and has passed an examination.
- Assessment includes:
- Determining readiness
- Determining the best power mobility base as well as:
- Seating
- Driving method
- Power seating
- Other features
The assessment includes determining readiness for a power wheelchair and encompasses all ages, particularly a pediatric audience. If you are interested in more information, check out some of our courses on pediatric power mobility. In addition to determining if a power wheelchair is appropriate for a client, we also need to determine the best power mobility base to match the individual's needs. This includes seating, the driving method, power seating, power base, and other features.
Power Operated Vehicles
- POVs: aka Scooters
- Features vs. power wheelchairs
- Consumer Preference
- Transport
- Maneuverability
- Stability
- Distance, power, and speed
- Motoric requirements
Let's talk about some of the features of a POV versus a power wheelchair. The first is consumer preference, and this is a huge one. Many people prefer a scooter because it is more aesthetically pleasing. Many people also gravitate towards scooters because they are more transportable as they break down into multiple pieces and can be placed easily in a trunk versus needing a modified van. The challenge is that once the scooter is taken apart it might be too much of a hassle to do so frequently.
Some scooters are more maneuverable than power wheelchairs, but the majority are not because of their large turning radius. Stability is also a concern as power wheelchairs tend to be less likely to tip than scooters, particularly a three-wheeled scooter. Scooters often cannot travel as far as power wheelchairs. Additionally, they may not have as much speed which can be important when ascending a hill or crossing the street before a light turns red. There are also different motoric requirements with a scooter than there are with a power wheelchair.
- Pros:
- Doesn’t look like a wheelchair
- Transportability
The advantage of a scooter is that it does not look like a wheelchair, and this can really be appealing to many of our clients. And, it is technically transportable. However, there are some drawbacks that are important for us to keep in mind.
- Cons
- 3 wheel scooters are more maneuverable, but also less stable and may tip
- 4 wheel scooters are more stable but have a very large turning radius
- Seating is limited
- Access
- Tiller
- Grip
- Transfers
- Less power, speed, distance
There are three and four-wheel scooters. The one pictured in Figure 1 is a four-wheel scooter.

Figure 1. Four-wheeled scooter by Pride Mobility.
Three-wheel scooters are more maneuverable, but they are also less stable and can tip, particularly when speeding or making a turn. For example, if you are driving across a slope, the scooter could tip. Four-wheel scooters are more stable, but they have a very large turning radius. As such, getting in and out of an elevator with a four-wheel scooter can be quite tricky. Seating is very limited on scooters. What you see in Figure 1 is typical of scooters. These are not designed for someone who requires a lot of postural support. A tiller is used to drive the scooter, and you can often move the tiller closer to the client. This is similar to a bicycle where you turn the handle back and forth, and speed is accomplished by squeezing a lever that is parallel to the handle. The client needs to be able to maintain their grip on the tiller to drive the scooter. Transfers can be tricky because the seat faces the platform where your feet are supported. Some of these have a seat that swivels to the side to allow the client to more readily transfer in and out. Finally, scooters typically have less power, speed, and travel distance on one charge as opposed to power wheelchairs.
Power Wheelchairs
- Drive wheel configuration
- Power seating
- Driving methods
- Programming
- Advanced features
- Training
With power wheelchairs, there are a number of factors that we need to keep in mind like the drive wheel configuration, power seating, driving methods, and programming. There are also some very advanced features available on these wheelchairs, and mobility training is needed to help optimize the driver's skills.
- Consumer Level
- Standard captain’s seat
- Joystick access
- Limited power seating
- Complex Rehab Level
- Full range of seating
- Frame growth and adjustments
- Full range of driving methods
- Full range of power seating options
- Advanced features
There are two main categories of power wheelchairs, Consumer Level, and Complex Rehab Level. A consumer-level wheelchair with a standard-style captain's seat can be seen in Figure 2.

Figure 2. Pride Mobility Jazzy Elite ES power wheelchair with a captain's seat.
These do not come in a lot of different sizes so it is important to make sure that seat depth is not too long for your client. These are driven by a standard joystick, and there are limited power seating options available such as a power tilt. These are appropriate for people who do not have complex postural needs.
Clients who require more advanced features would need complex rehab seating. Again, this requires a very skilled team to make sure that the features of the power wheelchair meet the parameters of that individual client. At the complex rehab level, there is a wide range of seating options from off-the-shelf cushions and backs to custom molded seating. There is also quite a bit of growth and adjustment in the frame to accommodate bodily changes or specific seating features such as a seat to back angle. There is also a full range of driving methods. For example, for people who are unable to use a joystick, there are dozens of different driving methods available. Additionally, there is a full range of power seating options that can be combined and a number of advanced features.
Drive Wheel Configuration
- Front
- Mid
- Rear
Let's start with the drive wheel configuration. Power wheelchairs are available in front, mid, and rear-wheel configurations, and we will go through each example.
Rear Wheel Drive
The first is rear wheel drive in Figure 3.

Figure 3. Example of a rear-wheel-drive power wheelchair.
A number of years ago, rear-wheel drive was very common but not as much now/
- Pros:
- Stability on all terrains
- Will handle downhill speeds with better control
- Wide range of choices
- Good for heavy outdoor use
- Fastest speeds
- Greatest available suspension
There are some advantages to a rear-wheel-drive configuration. In this configuration, the drive wheel sits behind the pelvis of the driver with a lot of chair in front of the client. These are very stable on a number of different terrains like grassy or bumpy areas. Additionally, if the client is going downhill at any speed, these tend to handle well. Often, other configurations feel less stable.
There is a wide range of rear-wheel-drive choices, are solid for heavy outdoor drivers, and provide the fastest speeds. Depending on the manufacturer, these also have the greatest available suspension to absorb the forces between the ground and the chair and client and reduce the vibration and jarring.
- Cons:
- Largest turning radius of the three configurations available
- Due to front caster placement, many front rigging options are limited (center mount)
One drawback to rear-wheel drive is that it has the largest turning radius of all three of the available configurations. Most doorways will allow manual and power wheelchairs, but what determines maneuverability is movement around furniture and within the home. The turning radius of a wheelchair is more than the actual footprint of the chair.
The other challenge with rear-wheel drive is that the front casters might interfere with the footplates particularly if the footplates are at a closed angle. As such, front rigging options could be limited because of this potential caster interference. There are a few wheelchairs that have a center mount option for the footplates, and this can sometimes reduce that caster interference.
Front-Wheel Drive
Next are front-wheel drive options as shown in Figure 4.

Figure 4. Example of a front-wheel drive.
In this case, the drive wheel is in front of the pelvis, and most of the wheelchair is behind the client. I work with a lot of children, and one client said, "It's like driving with a big butt." This is true as you have a lot of stuff behind you.
- Pros:
- Drive wheels pull the weight instead of push
- Improved obstacle climb capability
- With no front casters, can pull footplates closer to the body
- Small front turning radius
The drive wheels tend to pull the weight of the chair instead of pushing it. This is similar to when you have a front-wheel-drive car. These types of power wheelchairs have the ability to climb low obstacles due to the big wheel in front, but this climbing option depends on whether the front casters allow that. The front casters also are an anti-tip feature. Without large front casters, the footplates can be placed closer to the body. So, if someone needs their knees flexed at 90 degrees, this type of drive configuration will work for them. It also has a very small turning radius in the front as most of the chair is behind the individual. The individual can pull up to work surfaces and not have much of the wheelchair in the way.
- Cons:
- Less stable downhill
- Tendency to “fishtail” at faster speeds (downhill) or when being pushed by an attendant
- Forward tippy when client climbs on footrests
- Limited speeds unless compensated for in electronics
- Limits caregiver assist over curbs
- Limited suspension
One con with a front-wheel-drive configuration is that it is a little less stable going downhill. It also has a tendency to fishtail at faster speeds, particularly going downhill or when under rear attendant control. Fishtailing means that the back of the chair might wobble back and forth. This feature has improved over the years, but it can feel rather disconcerting to the driver. It can also be tippy forward if a client steps on the footplates. Despite warnings, many people use the footplates as a step stool. These do not always have the highest speed capability unless there is some compensation for that in the electronics. The reason for this is that the faster the wheelchair goes, the more likely we are to have a little of that fishtailing. Electronics can compensate and eliminate the fishtailing tendency. Caregivers may also have more difficulty assisting the client up and over a curb; whereas, in a rear-wheel drive, you can stand on the back a little bit to help pop up the front even though that is not technically recommended. The suspension is also somewhat limited in this configuration.
Center or Mid-Wheel Drive
Lastly, we have a center or mid-wheel drive as seen in Figure 5.

Figure 5. Example of a mid-wheel drive.
- Pros:
- Smallest possible footprint and turning radius
- Considered to be the most “intuitive” driving platform to some
- Very stable
These have the smallest possible footprint and turning radius which makes them very maneuverable. The drive wheel, even though it does not really look like it in this picture, sits right under the driver's pelvis making the maneuverability very intuitive. So, if I turn to one side or the other, I feel like I am turning on my own center of gravity in my own body space. This makes that easier to drive as there is not as much of the wheelchair in front or behind me. The mid-wheel drive also tends to be quite stable.
- Cons:
- May have challenges traversing through aggressive outdoor terrain
However, the center or mid-wheel drive does not always do as well on more aggressive outdoor terrain. There is a huge difference between consumer-level and complex rehab-level mid-wheel drive chairs. Consumer-level mid-wheel drive, which is very common, tends to be a little tippy and rocks backward when accelerating and forward when stopping. Consumer-level, mid-wheel wheelchairs are also notorious for lifting the mid-wheel off of the ground when going up a steep slope or ramp, but the complex rehab chairs in this category have addressed these issues.
Power Seating
- Tilt
- Recline
- Seat Elevator
- Elevating Legrests
- Standing
- Other
There are many power seating options available on power wheelchairs like tilt, recline, seat elevators, elevating leg rests, standing, and even more. We will go through each of these. Power seating is so important to keep in mind, even with children. If a child is old enough to understand how to drive a power chair, they should be old enough to understand when they might want to tilt, for example, to shift their weight. Some of these options can also be combined depending on individual clients' needs. Power seating needs to be ordered with the power chair so it is very important that we contribute to this area.
Let's now talk about each of these power seating functions and when they might be clinically indicated.
Power Tilt
- All angles stay the same: pelvis, knees, ankles
- The entire seating system tilts rearward (posteriorly), forward (anteriorly), or sideways (laterally) in space
The first is power tilt, and all the seated angles stay the same at the pelvis, the knees, and the ankles, and most commonly tilt moves rearward. An example can be seen in Figure 6.

Figure 6. Example of a posterior power tilt on a power wheelchair.
Figure 6 shows a posterior tilt, but we can also order an anterior tilt that goes forward or a lateral tilt that goes sideways.
- Pros
- Redistributes pressure
- Maintaining angles may inhibit muscle tone and maintain posture
- No shear forces
- Other assistive technology devices remain in position relative to the client
- Allows gravity to assist with trunk and head control
The advantage of tilt, and this is mostly in relation to a posterior tilt, is that we are redistributing pressure. When sitting upright, a great deal of the pressure is on the client's buttocks, posterior thighs, and some on the bottom of their feet and arms. A tilt redistributes the pressure by putting some of that on the posterior trunk and head by maintaining those seated angles. Tilting may also inhibit muscle tone. For some clients, if we open the seat to back angle like using a recline option, there can be increases in extension. To prevent this and still provide a weight shift, a tilt helps us to maintain the client's posture in relation to the support surfaces of the seating system.
There are also no shear forces. Whenever we recline or open a seatback angle, the client's body is going to move in relation to the support surfaces creating shear forces that can contribute to pressure injuries. If there are assistive technology devices that are mounted to the power wheelchair, such as a communication device, these are also going to remain in position relative to the client when using a tilt versus recline. And by using a posterior tilt, we can allow gravity to help us a bit with trunk and head control as gravity is not always our friend.
- Tilt systems accommodate contoured positioning systems and positioning systems with a fixed seat to back angle
- Range of motion limitations are accommodated
- Increases comfort for increased seating tolerance
- Provides a position of rest to address fatigue and post-seizure management
- May provide an improved position for swallow, visual regard, or functional tasks
Tilt systems, also accommodate contour positioning systems and positioning systems with a fixed seat to back angle. Some molded seating systems, like the one shown here by Aspen seating in Figure 7, are one-piece systems.

Figure 7. Example of Aspen seating system on a tilt.
Molded seating systems need to move as a whole and will not work with a recline. If we have a highly contoured system, even if it can work with recline, because of shear forces, the client may move out of alignment with the intimate contours which can lead to pressure concerns. If the client does not have an adequate range of motion (like in the hips) to handle a different type of power seating option such as recline, we do not have to worry about tilt as we are not changing those seated angles.
Tilt may increase comfort as the clients are able to change their position in space and increase their sitting tolerance. Thus, the client can stay in their wheelchair for a reasonable amount of time and have a position of rest. A tilt allows for the client to change their position throughout the day depending on the task. For example, I might use more of a task performance position if I am typing up a report, but if I am watching TV, I assume a more relaxed position. One of the challenges with wheelchair seating is that we need to choose one primary position to serve the client for functional activities, but with tilt, we can provide options and a position of rest. We can also improve their position for swallowing, vision, or any specific functional tasks.
Maintaining the hips in a fixed flexed position can have its own issues like a decrease in range of motion, a constriction of bowel and bladder function, particularly with the bladder, and catheter leaking.
- Cons
- Pressure relief is not as great as with recline systems
- Must move away from a work surface to tilt
- Items left on a tray will slide and fall
- Maintaining the hips in a flexed position can constrict the bladder
- A leg bag can leak during a tilt
What are the drawbacks of a power tilt? Pressure relief is not quite as high as when we are using a power recline. And, if I am tucked underneath a table like at a restaurant and I want to tilt, I need to move away from the table to tilt because otherwise, my knees are going to hit the bottom of the table. Additionally, if something is on a wheelchair tray, it is going to fall when I tilt.
- Lack of movement at hips and knees can lead to range of motion losses
- Some tilt systems have a higher seat to floor height than recline systems which can affect transfers and clearance under tables
That lack of movement at the hips and the knees can lead to range losses. Boy in a power wheelchair with a tilt is shown in Figure 8.

Figure 8. Example of a power wheelchair with a tilt feature.
Seating systems should provide as much independent control for the client to meet their postural needs, preserve range of motion, and maintain orthopedic alignment. Unfortunately, people who use wheelchair seating systems do begin to look more and more like their seating system meaning a loss of hip and knee extension. We need to provide alternative positions outside of the wheelchair to prevent some of this range loss like during sleep, by using a stander, et cetera. Some tilt systems have a higher seat-to-floor height than a reclined system. This height change can affect transfers as well as clearance under tables. This height measurement varies between manufacturers.
Anterior Tilt
- Anterior tilt can be used to provide an anterior slope to the thighs which in turn promotes pelvic stability and a slight anterior pelvic tilt
- Anterior tilt can be used to accommodate very limited hip flexion without the client leaning back too far
- Anterior tilt can be used to assist with transfers
An anterior tilt is shown in Figure 9 (in addition to a power elevator) and can be used to provide an anterior slope to the thighs to promote stability and a slight anterior pelvic tilt. Anterior tilt can also be used to accommodate someone who has very limited hip flexion without the client having to lean back too far. We can use a combination of a more open seat to back angle to accommodate that loss of range, but also anteriorly tilt the system. In this case, the client will be more upright and in a better position for transfers. You can see that if this woman needs assistance with a transfer, she is already halfway there.

Figure 9. Example of a client in an anterior tilt with a power elevator.
Lateral Tilt
- Lateral tilt can be used when a weight shift is required but the client cannot tolerate the head moving rearward past upright
- Lateral tilt can also be used to dynamically accommodate significant pelvic obliquity
Lateral tilt is not used very often and is not available from very many manufacturers. The one pictured here is available for Motion Concepts in Figure 10.

Figure 10. Example of a lateral tilt from Motion Concepts.
Lateral tilt can be used for weight shifts when the client cannot tolerate a posterior tilt because it creates postural insecurity or kicks off reflexive responses like extension. Lateral tilt can also be used to accommodate a very significant pelvic obliquity. Usually, we would handle a fixed public obliquity with a static wedge under the high side, but a lateral tilt gives us a dynamic option to accommodate for that.
Power Recline
- Open seat to back angle
- Typically includes a shear reduction feature which lowers the back as the back also reclines
- Often used in combination with elevating leg rests
- Often used in combination with tilt
Power recline, in comparison to a tilt, opens the seat to back angle as seen in Figure 11.

Figure 11. Example of recline with an open seat to back angle.
Typically, there is a shear reduction feature so that as the back reclines, it moves posteriorly as it also lowers. This posterior movement is crucial in a reclining system to minimize shear forces and keep the client in alignment with the support surfaces. There is nothing that completely eliminates shear, but this option greatly reduces it. Power recline is often used in combination with elevating leg rests, because it is not very comfortable to recline very far back without also extending the knees.
Recline can also be used in combination with tilt because with both options we can provide an even greater degree of pressure distribution and reduce pressure injury risk. We can also use this combination to help the client return to an upright position without a loss of pelvic position. We will look more closely at that in just a moment.
- Pros
- Easier catheterization, access to G-tube, diapering, clothes change
- Pressure redistribution
- Can do weight shifts at a work surface
What are the advantages of power recline? There are many instances where a recline may be needed like catheterization, G-tube feeding, or diaper or clothes change, especially out in the community. By reclining the individual, these tasks are can be completed without transferring the client out of the wheelchair.

Figure 12. Example of a recline on a Permobil F3.
Recline provides a great deal of pressure distribution as well. Instead of most of the pressure on the buttocks and the posterior thighs during a tilt, now we have pressure along the entire posterior aspect of the body. Recline redistributes the pressure over a greater portion of the body. And, if someone is tucked underneath the work surface like a desk, they should be able to do their weight shifts at their workstation.
- Pros
- Tray remains parallel to the floor
- May relieve orthostatic or postural hypotension
- Decrease in blood pressure relieved by lying down
- May relieve autonomic dysreflexia/hyperreflexia
- Increased blood pressure and other symptoms
- Treatment: weight shift, but keep head elevated
If they have a tray that is mounted to the seat rails of the chair, it will remain parallel to the floor and items will not slip off. Recline can also help with orthostatic or postural hypotension, a sudden decrease in blood pressure. When these conditions occur, it is important to lay the client back as soon as possible. Many of us have probably felt this when getting up too fast. You may feel dizzy and need to sit down for a minute. This condition is not uncommon in people with higher-level spinal cord injuries. Another condition that is sometimes seen in people with higher-level spinal cord injuries is autonomic dysreflexia or hyperreflexia, which is an increase in blood pressure and other symptoms. When this happens, the client needs a weight shift, but their head should remain elevated somewhat in relation to the heart (partial recline) which is a medical justification for power recline.
- Pros
- Passive range of motion at hips and knees
- A transfer may be easier
- Increased comfort, resulting in increased seating tolerance
- Provides a position of rest to address fatigue and post-seizure management
- Allows gravity to assist with trunk and head control
- May provide an improved position for swallow, visual regard, or functional tasks
Power recline may provide passive range of motion at the hips and knees. Transfers may also be easier depending on the surfaces like from the chair to bed. A reclining feature can provide increased comfort for the individual resulting in increased sitting tolerance. A recline can also create a position of rest to help address fatigue or to help someone recover from a seizure. It can allow gravity to assist with trunk and head control, and just like tilt, can have an impact on swallowing, vision, or various functional tasks.
- Cons
- Shear forces can disrupt the alignment
- Reclining increases pressure over the sacral area
- Opening seat to back angle can set off spasms
- May lead to a loss of seated position, making a return to upright difficult
- Cannot be used with a contoured positioning system
- Cannot be used by positioning systems with a fixed seat to back angle
There are some drawbacks to power recline as well. Depending on the individual, shear forces during reclining can disrupt alignment. Even though there is some technology built-in to prevent shear, there is some degree of shear during the movement of the back casing pressure over the sacral area. And as the client returns to an upright position, there might be a loss of that seated position. Opening the seat to back angle for some clients can set off extension and spasms. As such, recline cannot be used with a highly contoured or molded seating system because of the loss of position with those intimate contours. If the positioning system has a fixed seat to back angle, as some molded seating systems do, this obviously cannot support a recline feature.
- Clients with limited ROM at the hips or knees may be pulled out of position
- Reclining may affect the client’s ability to access other assistive technology devices
If the client has a limited range of motion at the hips or knees, they may be pulled out of position. This change in position may affect their access to mounted devices and impact their ability to control them. You can limit the degree of change in various power seating features via wheelchair programming. For example, if someone can only extend their knees by a certain degree, we could set a limit on the amount the elevating legrests could extend.
Tilt/Recline Combination
Tilt and recline can be combined. In this graphic from Permobil (Figure 13), you can see a wheelchair that is both reclining and tilting.

Figure 13. Permobil with both tilt and recline. Click here for an enlarged version.
Pros:
- Helps maintain posture, particularly on return to upright, while providing greater pressure relief through recline
- Client “tilts” while reclined to flex hips before coming forward from recline
Figure 14 shows a series of pictures highlighting the advantages of combining these two power features.

Figure 14. A power wheelchair with both tilt and recline.
One advantage is that we are maintaining the position of the pelvis. When a client is reclined and moves back to upright, the pelvis is often pushed forward into a posterior pelvic tilt. This is a big problem with recline. If the two technologies are combined, the person can be tilted while reclined (in the middle) to move their pelvis back into position. There is greater pressure relief when using recline, but by also utilizing the tilt, the position of the pelvis can be maintained.
- Cons:
- More weight
- More cost
- More complexity
- The client needs more control to operate these features than a single function.
Combining tilt and recline adds more weight to the chair. This is not typically an issue as these chairs weigh between 300 to 350 pounds, and you are not lifting this into the back of a vehicle. So, adding more weight is not always a big deal, but it is a consideration. And, adding both of these features costs more than simply a tilt or recline on its own. There's also more complexity to the system for caregivers or the client to go through, to manage these various power seating features. The client needs more control to operate these additional multiple features as compared to a single function.
Power Elevate
- Seating angles remain the same
- Seat to floor height increases
- Driving is usually possible while elevated
- Driving speed may be reduced while elevated
Let's talk about power elevate. In this case, as with tilt, the seating angles stay the same at the hips, knees, and ankles. The seat to floor height increases raising this person up. Driving is usually possible when elevated, but it might be slowed down. An example can be seen in Figure 15.

Figure 15. Example of a seat elevator.
This can be used to reach something out of a cupboard.
- Pros
- Extends functional reach
- Allows adjustment of seat to floor height to optimize transfers to various height surfaces
- Provides access to a variety of height work surfaces
- Vision
- Social interaction/participation
The advantage of power elevate is that it extends functional reach. Adjusting the seat to floor height can also optimize transfers to various heights surfaces like the bed, toilet, or stander. It also provides access to a variety of height work surfaces. I like this option for children. For example, kids in kindergarten sit at a lower desk, but by a few years, they move to a regular height student desk. They may also encounter different height surfaces in different classes like art or at home. All of these different height work surfaces work with a seat elevator.
This can also optimize vision. There are a lot of things that are difficult to see in the environment in a seated position. By raising them up, you can improve their visual regard for the environment. We know that with this power option social interaction and participation are greatly improved. People at a seated level are often overlooked, but when the person comes up to eye level, this dynamic changes. There is some really interesting research out there about that.
- Cons
- Challenging funding
- Limits power wheelchair base options
- May raise the seat to floor height, depending on the base
Now, one of the challenges with power elevator is that funding is very challenging, particularly through Medicare. There is some work being done on getting funding approval through Medicare, for both Power Stand and Power Elevate. We have to keep our fingers crossed on that one. Power elevate can sometimes limit the power wheelchair base options as only certain bases will accommodate these. And, the initial seat to floor height might be a little higher depending on the individual mobility base.
Power Elevating Leg Rests (ELRs)
- Usually used in combination with recline
- Can be programmed to move simultaneously with recline
This is usually used in combination with a recline and can be programmed to move simultaneously with the recline feature.
- Pros
- Passive range of motion to the knees
- May improve circulation and reduce edema
- If used in combination with a tilt to raise legs above the level of heart
An advantage of elevating leg rests is it provides passive range of motion to the knees which can improve circulation. An example is seen in Figure 16.

Figure 16. Example of elevating leg rests on a Quickie S-626.
Another common reason for using elevating leg rests is to reduce edema. However, it is important to remember that this will only work if the legs are higher than their heart. Thus, we need to combine this with a tilt system so that the feet, when elevated, are truly higher than the heart. Some of our clients will not tolerate that position as it feels like they are falling. If that is the case, we might instead transfer the client to bed for periods of time.
- Cons
- Can pull the pelvis forward into posterior pelvic tilt if hamstrings are tight
The main drawback of using elevating leg rests is that if the client does not have enough range of motion due to tight hamstrings the client's pelvis will be pulled forward. This is because hamstrings are attached to the pelvis and the knees. Again, we can use programming to limit how far the elevating leg rests go.
Power Stand
- Hips and knees extend partially or fully
Here is an example of power stand.

Figure 17. Permobil F3
Here the hips and knees extend either fully or partially. They do not need to extend a hundred percent for someone to be able to use the standing feature.
- Pros
- Many physiological benefits of standing
- Standing from a wheelchair:
- Extends functional reach
- Improves visual field
- Improves social interaction/participation
- Increases compliance with a standing program
There are many physiological benefits to standing like improving functional reach, visual field, and social participation. Perhaps, this person has a stationary stander, but they are not keen on getting in it. In fact, most people who have a stander on a power chair will assume this position for longer periods of time than those who only have a stationary stander.
- Cons
- Client must have an adequate range of motion
- Client must have medical clearance for standing
- Risk of fracture
- Autonomic issues
The client has to have an adequate range of motion to benefit from a stander, and you can limit how far this system extends. The client must also have medical clearance for standing. Clients who have not stood for 20 years may have osteoporosis and are at risk of a fracture. There can also be autonomic functions that are not accommodated to an upright position. I check in with the physician and ask for medical clearance for standing just like we would do other therapeutic situations. I might also start a client out slowly and build up to a standing position to avoid medical consequences.
Driving Methods
There are a number of driving methods available. There are courses on proportional and non-proportional driving methods on this site. This is Jonathan using a head array in Figure 18, which is a non-proportional driving method.

Figure 18. Non-proportional driving with a head array.
It allows people who cannot use a standard joystick to continue to be independent in their mobility.
- Proportional (analog)
- Non-Proportional (digital)
We have two main categories of driving methods, proportional, and non-proportional.
Proportional Access
- Joysticks and a few others
- Requires grading of force and distance of movement
- 360-degree control
- Speed control
Proportional access is almost all done with joysticks, including mini proportional joysticks, which can be used by the hand or the chin.

Figure 19. A standard and mini-joystick.
Proportional alternative driving methods require grading of force and distance of movement. This means that the client has to reach out and get the driving device to the right spot, not overshoot or undershoot the target. The further the joystick is deflected from the center, the faster the chair will go. These can also provide up to 360 degrees of directional control as long as the client has that ability.
Non-Proportional Access
- Basically, using 1-5 switches to control the direction of the chair
There are many alternative driving methods that fall under the non-proportional access category. They can use one to five switches to control the direction of the chair. There is forward, left, right, and reverse. And, if I am able to activate forward and right at the same time, they can get a more subtle course correction. The fifth switch is a mode switch that tells the wheelchair the client is going to do something else besides drive. They may send a signal to their power seating. Or, if the client only has four switch sites available on their body, you can make the fourth one the mode switch and use the mode switch to also access reverse as well as other features like that power seating. Here are just some examples of the many different options there are in Figure 20. And again, I would encourage you to check out our webinar on Non-Proportional Driving Methods.
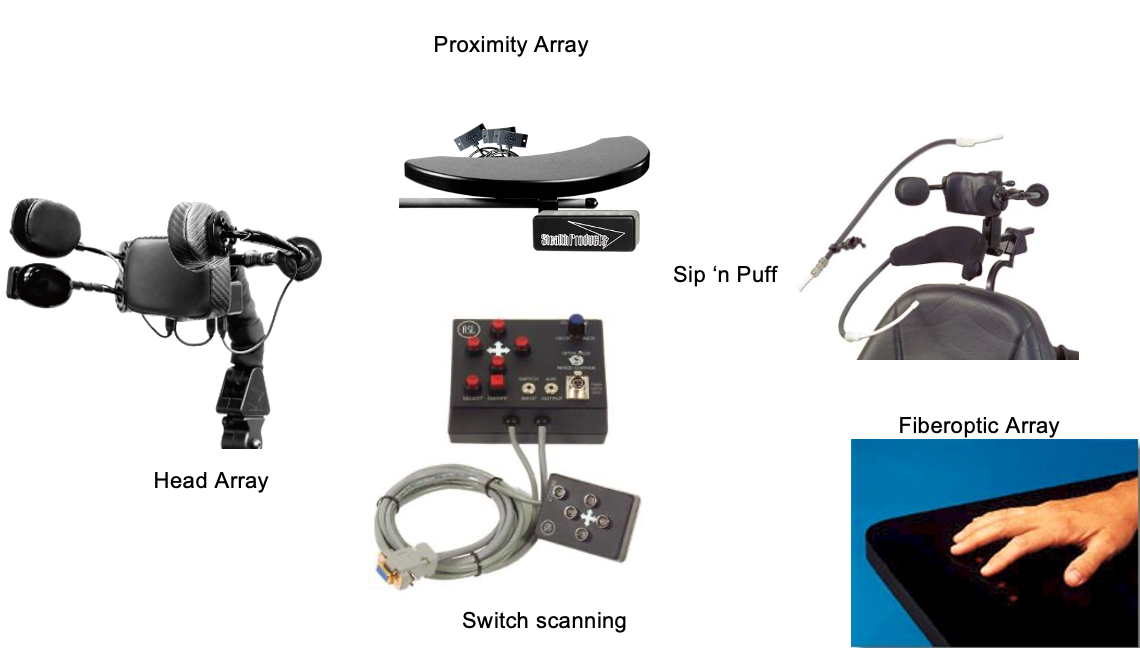
Figure 20. Examples of non-proportional access controllers.
Programming
- Optimizes drive performance and efficiency
- Enables control of other features such as speed, reverse, and actuators through the drive control
Programming is a rather complex topic and can be done by the supplier or clinician. Sometimes, it is a team effort. Programming optimizes the drive performance and efficiency of the chair. It also can be utilized to enable control of other features through the driving method, such as control speed, reverse, and actuators, another word for power seating. Power wheelchair companies use a certain electronic system, and each of those electronic systems has their own unique programmer, such as R-Net pictured in Figure 21.

Figure 21. Example of an R-Net controller.
Advanced Features
- Power wheelchairs do much more than drive!
- Power seating
- Bluetooth transmission to control a communication device, computer, tablet, or smartphone through the driving method
Then, we have advanced features. Again, there is an entire webinar that goes over some of these advanced power wheelchair features. It is important to remember that power wheelchairs do a lot more than drive. They can support the control of power seating through the driving method. There is also Bluetooth transmission that allows the driving method to control a smartphone, a tablet, or a communication device. It is quite amazing what can be supported by these chairs. Examples are shown in Figure 22.

Figure 22. Examples of advanced features on a power wheelchair.
- Interfacing allows an external assistive technology device to be controlled through the driving method without Bluetooth
We can also utilize interfacing but this requires some additional electronics. It is another method of allowing control of interface devices like a communication device without Bluetooth. Bluetooth is sometimes standard on these power chairs, and sometimes it is an add-on optional feature. It may be cheaper to add on Bluetooth capabilities and then add on the interfacing component. Figure 23 shows an interfacing component.

Figure 23. Interfacing component.
- Smart wheelchair technologies
- New technologies to make power wheelchairs smarter
- Collision avoidance, drop-off detection
- Tip warnings
- More
Smart wheelchair technologies are new emerging technologies that include sensors on the wheelchair to help the driver to avoid collision with obstacles around them. For example, a client can go through a doorway without running into the sides of the doorway. There is also drop-off detection so that the chair will not go over a curb. There may be a warning when on a steeper incline to let the client know that they are at risk of tipping. These are exciting changes in power wheelchair technology. The main commercially available option right now is LUCI. If you are interested in more information about smart wheelchairs, you might want to go to luci.com.
Pediatric Power Mobility
- Research has demonstrated that early mobility is key to overall vision, cognitive, and psychosocial development.
- Augmented mobility
We have other course offerings addressing pediatric power specifically, but I do want to touch on a few things. Research has demonstrated that the provision of power mobility at a young age is important across many developmental areas. We want to make sure that we are building those brain cells in our clients. There are also augmented mobility options such as adapted ride-on cars that are used sometimes in the pediatric population. Again, this is more for the developmental benefit than functional mobility. Figure 24 shows a young child in a power wheelchair.

Figure 24. Young child in a power wheelchair.
Mobility Training
- Pre-mobility training develops skills required to use a power wheelchair
- Mobility training optimizes driving skills
- New technologies for power wheelchair assessment and training
- Virtual Reality
Mobility training is something that is also important to keep in mind. Pre-mobility training can develop skills that are required to use a power chair before we even get to the evaluation. Mobility training after the power wheelchair can optimize driving skills. There are even some new emerging technologies for power wheelchairs, assessment, and training. These include virtual reality where the client can use virtual reality goggles or look at a monitor if goggles are not tolerated. This is yet another tool in our toolbox for providing power wheelchair assessment and training.
Take-home Message
What is our take-home message here today? Power mobility can be complicated. Assessment is a team activity including the supplier. We need to collaborate to get the best recommendation for an individual. Power mobility can provide independent mobility to clients who otherwise are dependent or inefficient with their mobility. There are a lot of driving methods to support an individual's needs. I would encourage you to check out some of the other courses on power mobility.
Resources
- RESNA Position Papers:
- The Application of Pediatric Power
- The Application of Seat Elevating Devices
- The Application of Tilt, Recline, and Elevating Legrests for Wheelchairs
- The Application of Wheelchair Standing Devices
- RESNA Wheelchair Service Provision Guide
- www.RESNA.org
I also want to direct you to some resources that might be helpful. RESNA has a series of position papers that address what the literature supports in this area of intervention and what the clinical guidelines are for pediatric power and a whole host of different power seating interventions. These are all available on the RESNA website.
- Access to Independence Resources
- Indoor Power Mobility Criteria
- Outdoor Power Mobility Criteria
- Pre-mobility Training Guidelines
- Mobility Training Guidelines
- Complex Rehab Power Wheelchair Electronics Comparison Chart
- More
- www.atilange.com/Resources
I also have these free resources on my website, under the resources tab. Feel free to download and use any of them that you would like if they are helpful to you.
Hands-on Activity
I have a hands-on activity suggestion for you. Contact a Seating and Mobility Clinic in your area and arrange to observe a power mobility evaluation. It is an awesome learning activity, and most people who work in this field will be very happy to have you join them. I want to thank you very much for your time here today.
Questions and Answers
Is it recommended to train caregivers to help with realignment after changing a patient's position or does a positioning fix itself when the patient returns to an upright position?
That is a great question. Many of our clients could certainly benefit from being repositioned throughout the day. One of the goals of combining recline and tilt together is that the client can do as many weight shifts as they would like during the day for comfort, function, and pressure relief. It is important for the client to not be dependent on someone else to reposition them every time they shift their weight.
A great deal of this is also dependent on the seating system itself. If the seating system is supporting someone correctly, then hopefully they are less likely to lose position. However, we do know that a recline does tend to pull the pelvis into a posterior pelvic tilt. Thus, it is always very important to train caregivers to make sure the client is positioned within their seating system correctly from the beginning and monitor that throughout the day.
Is the power elevate primarily used with mid-wheel drive wheelchairs, or can it be used on others?
It can be used on all three drivewheel configurations. It can be used in combination with other power seating features.
My student recently received a power wheelchair with a head array and custom seating. The student has a lot of contractions in the upper and lower extremities. The control center programmer comes off the front seat and angles up. Do you have any recommendations for protecting the programmer? I am worried about the student bumping it.
A non-proportional driving method usually has a display that is often placed in front of the client. It is fragile and needs to be mounted within the footprint of the chair. So, I would start by making sure it is mounted within the footprint of the chair and not sticking out. If it is on some type of a gooseneck mount and moving, you may want to switch it out to a more stable mount. You can also mount the display behind the client if they do not need to access it.
Can you talk about replacement wheelchairs for adult patients?
The replacement of a power chair depends on the individual funding source. We used to think it was five years, but most funding sources now are making us demonstrate that the power wheelchair needs to be replaced after this number of years even if the chair was quite old. Similar to an old car, we may have to spec out with the supplier the cost to replace the parts to decide if a new wheelchair is the best option.
Citation:
Lange, M. (2021). Power wheelchairs. PhysicalTherapy.com, Article 4829. Available at www.PhysicalTherapy.com
